

As women we are workers, consumers, reproducers, sexual objects, desired and detested. For all these reasons we use the health system more than men. We have children, we get over-tired, we need medication. We have to care for sick children. We need contraception, abortion. We consume vast amounts of chemical beauty products in order to make ourselves desirable to men. We are beaten and raped and then need to be cared for. Yet health systems are nearly always in the hands of men. Men have successively taken over the domain of medicine. It is they who are the doctors in most countries. It is they who have developed the drug industry into the enormity it is today, and it is they who make the laws on health. Doctors, pharmaceutical industries, governments: this is a powerful tripartite alliance.
In our survey of the literature we found much on pharmaceuticals, but almost nothing written from a feminist perspective. We also began to realize the importance of the alliance between drug companies, doctors and governments. The first piece in this section is therefore a contribution by Isis. We broadly examine (a) the power of the pharmaceutical industry and its relationship to women, (b) the domination of the medical profession by men and the historical reasons for that, and (c) the relationship between drugs, doctors and governments, and what that can mean for women. We see it as a piece which begins to raise some questions in a highly complex domain.
The other articles in this section elaborate on more specific aspects the question, who controls women's health ?
Pharmaceutical (drug) companies
"The pharmaceutical industry is one of the most profitable in the world. Since the mid 1950's it has consistently recorded profits that are substantially higher than the average for all industry in both the USA and the UK (United Kingdom), and was often the most profitable manufacturing industry". The growth of the multinational drug companies dates from the 1940's and 50's when expansion of the petrochemical industry on which they are based was at its most rapid. At first many small companies mushroomed, but these have since been swallowed up to the point where, for instance, in Britain, five companies control 30% of the market, in the USA ten companies control over 40%, and the three Swiss firms, Hoffmann-La Roche, Sandoz and Ciba-Geigy account for some 15°/o of world sales (see list below).
The structure of the industry is highly complex, since, like all multinationals, these companies have branched out from the simple manufacture of chemical-based medicines. They are now involved in producing and marketing everything from fertilizers, insecticides and special kinds of food grains, to soaps, detergents, cosmetics and perfumes. They are as much involved in making products for chemical welfare (defoliants, herbicides, etc.) as vitamins and baby foods.
The direct impact of drug companies' activities on women's daily lives is thus enormous. In July 1976 an explosion caused by the faulty operating of the only safety valve at the ICMESA chemical plant in Seveso, Northern Italy, spread a huge noxious black cloud over the area. After 20 days 46 people had been hospitalized, and at the end of two months, an area of nearly 350 hectares was declared contaminated and more than 2,000 people were evacuated. It was announced that the poison which had escaped was dioxine, one of the most dangerous chemicals in the world. used by the US army as a defoliant during the Vietnam war. The effects of dioxine are slow and long-lasting, sometimes only becoming evident after one generation. It penetrates the skin, the blood, the liver, the kidneys, the stomach, the lungs and the central nervous system. It causes cancer and genetic mutations (changes in the species). It also attacks pregnant women and their unborn babies. Several women from Seveso managed to get abortions in spite of the antiabortion law then in force in Italy. Other pregnant women were prevented from having abortions by the Church. One woman gave birth to a stillborn baby without a brain, and children born since have suffered from stomach abnormalities. The full effects of this contamination will only be known after 20-25 years. In the meantime the women from Seveso wonder constantly whether they should have children or not. ICMESA is a subsidiary of Givaudan, a Swiss chemical and cosmetic manufacturer owned by Hoffmann-La Roche, the biggest pharmaceutical company in the world, best known for its top-selling tranquilizers, Librium and Valium.2
Cases like this show how women end up suffering more and bearing more of the consequences of pharmaceutical companies' activities, because of their role as mothers and carers of people in the community. They are also the major consumers of health services. This means that the effects of the kinds of drugs marketed are of direct concern to women. You may be interested to know that :
- Conmel (manufactured by Winthrop, USA), a painkiller which can cause fatal blood diseases, is banned in the USA except as a last resort medicine. Yet it has been found in Brazil with a packet insert suggesting that the drug be used for "migraine headaches, neuralgia, muscular or articular rheumatism, hepatic or renal colic, pain with fever which usually accompanies grippe, angina, otitis, sinusitis or tooth extraction".
- Ritalin (Ciba-Geigy, Switzerland), an antidepressant often prescribed for "minimal brain dysfunction" in children, leads to hyperactivity, a form of acute nerve stimulation involving rapid breathing and a rise in heart pressure.
- Birth control pills (many companies), a drug for women against pregnancy, were originally tested on poor Puerto Rican and Mexican women in the 1950's. Found to cause numerous side effects including nausea, headaches, persistent bleeding, sore breasts, weight gain and loss, heart disease and cancer. Although they have been improved since, recent studies show that birth control pills are still related to a higher incidence of heart attacks and cancer.
- Depo-Provera (Upjohn, USA), an injectable contraceptive for women. Although banned in the USA because it causes breast and cervical cancer in animals, it is widely marketed elsewhere, especially in countries of the Third World (see ISIS Bulletin No. 4). Reasons given for this are (a) distribution of health services is poor in many parts of the developing world, so that it is a distinct advantage if women are either too stupid or lazy to understand and deal with other methods of contraception, and when fertility control is of major importance, an injectable which solves the problem easily is worth the risk of cancer.
These are just a few examples from a long list of dangerous drugs that have been used sometimes indiscriminately and frequently without proper controls. In the case of contraceptives, experiments are directly carried out on women - mostly poor women from Third World countries.^ Some countries, like the USA, the UK and those of Scandinavia, have set up organizations whose purpose is to make sure that strict controls are kept on the manufacture and use of drugs. But drugs are a profitable business, so if they cannot be marketed in one country, companies will market them in another, as the above examples show.
This is a small indication of the unscrupulousness of the Industry - their concern for profits rather than people's health and well-being. In fact we might wonder whether the pharmaceutical industry has much to do with health at all. When we know that the UN World Health Organization's model list of essential drugs numbers around 100^, and yet currently several thousand varieties of brands are marketed internationally, we should think long and hard about what we are doing when we ask for and buy drugs. Because of their vast profits and domination of the world market, pharmaceutical companies actually dictate priorities in health (or sickness) by deciding which drugs they are going to concentrate on researching and marketing. Companies will only invest in drugs which will sell widely and bring good returns. This means (a) they develop drugs for "rich country" diseases such as heart complaints, depression, insomnia, ulcers and cancer (frequently research consists of inventing "me too" drugs which are simply one company's answer to a similar drug manufactured by another company) and (b) the poor country diseases will be overlooked unless there is likely to be a long-term profit, as with birth control pills and injections, for the "population disease". Indeed, contraception is one area of research where priorities are not only set by the industry but are carried out by men on and for women. Oral and injectable contraceptives are much more expensive than barrier methods, and so more profitable. They also are much more dangerous. Research done on male contraception is minimal (see Judy Norsigian's article below)
As consumers of health care we may not be aware of the' profound influence of the pharmaceutical industry, since when we are sick, we go to the doctor. But it is important that we understand the mechanisms at work. This extract from the Concerned Rush Students^ shows just how subtle these mechanisms are.
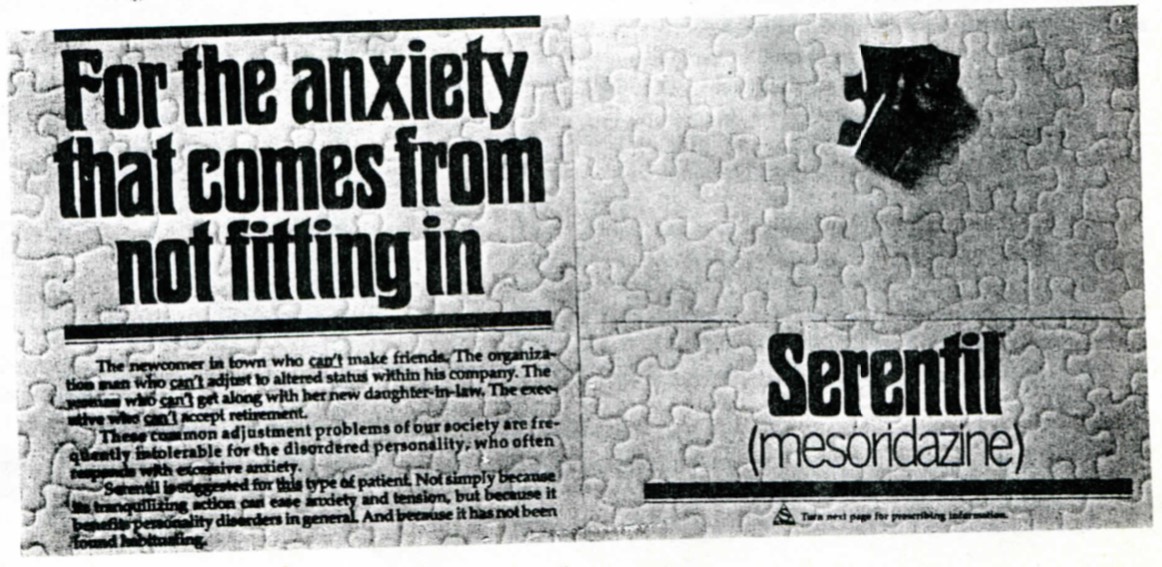 Another significant feature to investigate is the turning of non-medical problems into medical ones requiring drug therapy. On the one hand this represents merely an extension of the never-ending search for new markets. More important that this quantitative expansion, though, is the entrance of the drug industry into a new realm of our daily lives; we see this as a form of social control . A 1971 medical journal advertisement for the Sandoz tranquilizer Serentil illustrates this trend:
Another significant feature to investigate is the turning of non-medical problems into medical ones requiring drug therapy. On the one hand this represents merely an extension of the never-ending search for new markets. More important that this quantitative expansion, though, is the entrance of the drug industry into a new realm of our daily lives; we see this as a form of social control . A 1971 medical journal advertisement for the Sandoz tranquilizer Serentil illustrates this trend:
The thrust of this ad is to define the tensions of everyday life in our society as pathological. By extending the usage of drugs to include what are universal experiences, the potential market for the drugs becomes unlimited. The success of this campaign should not be underestimated. As contrived as the above example and others like it seem, the products they are promoting sell : psychoactive drugs are now the most heavily prescribed drugs in the US
The industry's massive campaign urges people to consume drugs as the answer to the alienation of work and home life. (...) Merck's combination phenothiazine antidepressant Triavil (perphenazine-amitriptyline) is for those patients who have lately felt "sad or unhappy about the future ... easily tired and who have had difficulty in making decisions, difficulty working." Triavil also treats "the empty nest syndrome, allowing the menopausal-aged woman to cope successfully ... after the children are grown and gone." (...)
The favourite anxiety producing situations depicted over and over again are problems of work (or lack of it), marital conflicts, aging difficulties, and deterioration of urban life. We hardly feel these problems were invented by the drug industry. In fact we would agree with the industry that these problems reflect the major issues facing people in the United States. Today, as these conflicts generated by our country's social, political, and economic policies are becoming more intense, the trend toward the "drugging" of the American people becomes increasingly significant. (...)
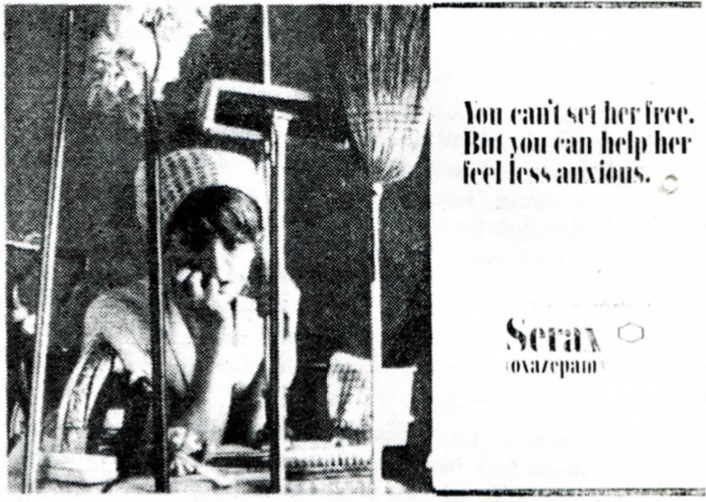 67% of psychoactive drugs are given to women. Each year 1/3 of the women over the age of 30 receive prescription tranquilizers, stimulants, and/or antidepressants. These statistics are significant because they reflect society's failures to meet the needs of women. Forced to cope with low-paying, unfulfilling jobs, the burden of family and child care, and never ending housework, women often present doctors with vague complaints of pressures frustrations, and anxiety. Since 90°/o of US physicians are men, the doctor is are then reinforce by a drug industry which supports sex role stereotypes and presents the oppressive reality of women's lives as an unchangeable fact of life :
67% of psychoactive drugs are given to women. Each year 1/3 of the women over the age of 30 receive prescription tranquilizers, stimulants, and/or antidepressants. These statistics are significant because they reflect society's failures to meet the needs of women. Forced to cope with low-paying, unfulfilling jobs, the burden of family and child care, and never ending housework, women often present doctors with vague complaints of pressures frustrations, and anxiety. Since 90°/o of US physicians are men, the doctor is are then reinforce by a drug industry which supports sex role stereotypes and presents the oppressive reality of women's lives as an unchangeable fact of life :
But the drug company helps to enslave her ! Drug ads portray women either as hypochondriacal housewives or as sex objects to titillate the fantasies of male physicians. In this way the drug industry contributes to, rather than relieves, the oppression of women.
So doctors work hand in hand with the industry, and very often become nothing more than their agents
The medical profession
Quite apart from the tremendous influence on it by the drug companies, the medical profession has its own prestige, built up over several centuries. This prestige, and indeed the transformation of healing into a "profession" has been created by a long struggle from which men emerge dominant :
Women have always been healers. They were the unlicensed doctors and anatomists of western history. They were abortionists, nurses and counselors. They were pharmacists, cultivating healing herbs and exchanging the secrets of their uses. They were mid-wives, traveling from home to home and village to village. For centuries women were doctors without degrees, barred from books and lectures, learning from each other, and passing on experience from neighbor to neighbor and mother to daughter. They were called "wise women" by the people, witches or charlatans by the authorities. Medicine is part of our heritage as women, our history, our birthright.
Today, however, health care is the property of male professionals. Ninety-nine percent of the doctors in the US are men; and almost all the top directors and administrators of health institutions. Women are still in the overall majority - 70 percent of health workers are women — but we have been incorporated as workers into an Indus try where the bosses are men. We are no longer independent practitioners, known by our own names, for our own work. We are, for the most part, institutional fixtures filling faceless job slots : clerk, dietary aid, technician, maid. (...)
 We are told that our subservience is biologically ordained : women are inherently nurse-like and not doctor-like. Sometimes we even try to console ourselves with the theory that we were defeated by anatomy before we were defeated by men, that women have been so trapped by the cycles of menstruation and reproduction that they have never been free and creative agents outside their homes. Another myth, fostered by conventional medical histories, is that male professionals won out on the strength of their superior technology. According to these accounts, (male) science more or less automatically replaced (female) superstition - which from then on was called "old wives' tales".
We are told that our subservience is biologically ordained : women are inherently nurse-like and not doctor-like. Sometimes we even try to console ourselves with the theory that we were defeated by anatomy before we were defeated by men, that women have been so trapped by the cycles of menstruation and reproduction that they have never been free and creative agents outside their homes. Another myth, fostered by conventional medical histories, is that male professionals won out on the strength of their superior technology. According to these accounts, (male) science more or less automatically replaced (female) superstition - which from then on was called "old wives' tales".
But history belies these theories. Women have been autonomous healers, often the only healers for women and the poor. And we found, in the periods we have studied. that, if anything, i was the male professionals who clung to untested doctrines and ritualistic practices - and it was the women healers who represented a more humane, empirical approach to healing. (...)
The suppression of women health workers and the rise to dominance of male professionals was not a "natural" science, nor was it the result of women's failure to take on healing work. It was an active takeover by male professionals. And it was not science that enabled men to win out : The critical battles took place long before the development of modern scientific technology.
The stakes of the struggle were high : Political and economic monopolization of medicine meant control over its institutional organizations, its theory and practice, its profits and prestige. And the stakes are even higher today, when total control of medicine means potential power to determine who will live and will die, who is fertile and who is sterile, who is "mad" and who is sane.
The suppression of female healers by the medical establishment was a political struggle, first, in that it is part of the history of sex struggle in general. The status of women healers has risen and fallen with the status of women. When women healers were attacked, they were attacked as Women; when they fought back, they fought back in solidarity with all women.
It was a political struggle, second, in that it was part of a class struggle. Women healers were people's doctors, and their medicine was part of a people's subculture. To this very day women's medical practice has thrived in the midst of rebellious lower class movements which have struggled to be free from the established authorities. Male professionals, on the other hand, served the ruling class - both medically and politically. Their interests have been advanced by the universities, the philanthropic foundations and the law. They owe their victory - not so much to their own efforts - but to the intervention of the ruling class they served.
In many Third World countries, the health system has developed from the Western male-dominated services brought by the colonizers for their own use. This means that large sophisticated hospitals have been built which must be run by people who receive training in the West. This has produced an absurd situation where, in West Africa, for instance, a doctor's training costs the equivalent of a peasant's income for 100-200 years.8 These people are, of course nearly always men. Thus, when he has finished this training, the doc tor finds it totally inappropriate to the problems he has to deal with in the country, both because it is too technical and because it does not apply to the people who need healthcare most — malnourished women and children. He has be come a member of a privileged class, removed both by Western training which is in any case sexist and based on ; language foreign to the indigenous population, and by the position he gets in the hierarchical health system in his own country (based on Western models). Women in Third World countries are the particular victims of this medical classicism sexism since (a) they use the services more because of the role in childbearing and caring, and (b) a high proportion c them are illiterate. The article on Public Health Services i Morocco reproduced below, details this aspect fully.
In the West, most women are not illiterate, but the prestige of the medical profession still keeps us in awe. We often c' not know what is wrong with us until we have been to doctor (a measure of our ignorance of our bodies), and v expect the doctor to give us pills. In 1974, doctors in Brit; wrote an average six prescriptions for every woman, man and child.
Governments
Clearly governments are also implicated in this situation, many ex-colonies of the Third World, the colonial legacy leaves them increasingly dependent on the pharmaceutical industries as employers, investors and sources of taxable venue. They receive aid in the form of hospitals, research units and trained personnel from the rich countries. In Bangladesh "90% of the Government spending on health g to 6% of the people, and the wealthiest are found in r 6%, not the poorest. Medical students are still trained meet the needs and stresses of the wealthy, and are tau nothing of the so-called "tropical diseases" more correctly termed "diseases of the poor". In Tanzania, spending on drugs now accounts for 22% of the Tanzanian Health Ministry's allocation, compared with 11°/o in Britain.
It is important to note, though, that this is a feature of v are called market economy (capitalist) countries, both in developing and the developed world. In centrally-planned (socialist) countries, the situation can be very different Countries like the Democratic Republic of Vietnam or Mozambique have made conscious policies to reach the rural population. The former, for example (population 18-19 lion), after ten years of independence has 35,000 health instructors of various grades. In Tanzania (population 1 million) which is following a capitalist health system, i are only 323 health instructors after the same period Cuba and China are probably the best examples. Health services there not only reach nearly the entire population they are set up on a non- hierarchical basis. This mean^ health workers do not have more prestige than other people in the community. They work with people and from their own situations and experiences. This can have big implications for women since it means that health is no longer necessarily a male-dominated "professional" domain. There are not the sexist divisions between "nurse" and "doctor". The question of literacy does not count in getting health care.
Yet the popularising of health care on the socialist models not necessarily enough, as we know. Socialism has not been formulated by women, so there is no reason to think that women will necessarily be taken into account either as health workers or as users of the system. But we can use these experiences to help change our reality.